
Today, 21 women will die of a gynaecological cancer, and 60 women will be diagnosed.
Understanding the symptoms, getting the HPV vaccine, and attending cervical screening when you're invited are three of the most powerful things you can do to change those numbers — for yourself and the women around you.
That's why we're calling on you to talk more openly about these life-saving issues.
To jump to a specific topic, please use the links below:
gynaecological
cancers,the HPV Vaccine, and cervical screening
Cervical cancer
Ovarian cancer
vaginal cancer
vulvaL cancer
womb (uterine) cancer
Are you looking for our
downloadable resources?
cervical cancer
This is probably the one you are most familiar with! Cervical cancer can be found anywhere in the cervix, which is the opening between the vagina and the womb. Nearly all cervical cancers are caused by an infection with certain high-risk types of human papillomavirus (HPV). You cannot always prevent cervical cancer, but cervical screening and HPV vaccination are the best ways to protect yourself from this kind of cancer.
Around 3,300 women are diagnosed with cervical cancer in the UK each year, most commonly diagnosed between 30 and 35 years.
-
Around 3,300 women and people with a cervix are diagnosed with cervical cancer in the UK each year, and the most common age of diagnosis is between 30 and 35 years old.
-
The most common symptoms of cervical cancer are:
Vaginal bleeding that's unusual for you – including bleeding between periods, during or after sex, or after the menopause, or having heavier periods than usual
Changes to your vaginal discharge
Pain or discomfort during sex
Pain in your lower back, pelvis (between your hip bones), or lower tummy
If you have any of the symptoms listed above, particularly if:
They are not normal for you
They are persistent
There are repeated episodes
They do not go away
…be sure to visit your GP for a check-up.
Remember, these symptoms are very common and can be caused by many different conditions — most women with symptoms like these do not have cancer. But your awareness of your body is the first and most important step, and early diagnosis can save lives.
-
Human papillomavirus (HPV) is the major cause of cervical cancer — nearly all cervical cancers are caused by infection with certain high-risk types of HPV. HPV is passed on through sexual contact.
All children, both boys and girls, aged 12 or 13 in the UK are routinely offered the HPV vaccine at school in Year 8 — since September 2023, this is given as a single dose. If you missed it at school, you can get the HPV vaccine for free on the NHS up to your 25th birthday. The vaccine protects against the strains of HPV most likely to cause cervical cancer, and has already cut cervical cancer rates in young women in England by almost 90%.
Other risk factors include smoking, having a weakened immune system (for example from HIV or AIDS), and taking the contraceptive pill for more than 5 years. Women who have given birth to multiple children, or who had children at an early age (under 17), are also more likely to get cervical cancer.
*Risk factors are characteristics at the biological, psychological, family, community, or cultural level that precede and are associated with a higher likelihood of negative outcomes.
-
Treatment for abnormal cervical cells
There are several different treatments available for precancerous changes in the cervix. They all aim to remove or destroy the abnormal cells.
The most common treatment in the UK is LLETZ (large loop excision of the transformation zone), where a thin heated wire loop is used to remove the affected area. It's usually carried out under local anaesthetic at the same time as a colposcopy and takes around 15 minutes, with no overnight hospital stay needed. Other treatments include a cone biopsy (where a cone-shaped piece of tissue is removed, usually under general anaesthetic) and, less commonly, treatments that destroy the abnormal cells using heat or cold.
In rare cases — for example, if you are past your menopause, have had all the children you want, or have had severe or repeated abnormalities — your doctor may suggest removing the whole of your womb (a hysterectomy). This does not mean you have cervical cancer, but that the abnormal cells on your cervix are closer to becoming cancerous.
Treatment for cervical cancer
Cervical cancer is often treatable, especially if found early. Your treatment plan will depend on the size and type of cancer, where it is, whether it has spread, and your general health. It will usually involve surgery, chemotherapy or radiotherapy, and may also include targeted medicines or immunotherapy.
Surgery is often the main treatment when cervical cancer is found early. Depending on the size and spread of the cancer, this may involve removing only part of the cervix, the cervix and upper vagina (a trachelectomy — fertility-sparing surgery that allows future pregnancy), or the cervix and womb together (a hysterectomy). In some cases, lymph nodes or other surrounding tissue may also need to be removed.
More advanced cervical cancer is usually treated with chemotherapy and radiotherapy together (chemoradiotherapy), or with chemotherapy alone. Radiotherapy may also be given after surgery to lower the risk of the cancer coming back, or to help relieve symptoms such as bleeding. For advanced cancer that has come back or spread, targeted medicines and immunotherapy may also be used.
Even if cervical cancer cannot be cured, treatments are available to control symptoms and help you live longer and more comfortably. Your specialist care team will work with you to create a treatment plan that's right for you.
-
Cervical screening is essential in combatting cervical cancer!
The NHS Cervical Screening Programme offers testing to women and people with a cervix between the ages of 25 and 64. You'll usually be invited every 5 years, or sooner (typically every 1 to 3 years) if you've previously had an abnormal result or high-risk HPV detected.
In 2023–24, over 5 million people aged 25 to 64 were invited for cervical screening (sometimes called a 'smear test') in England.
Around 13 in every 100 people screened will receive a result that detects high-risk HPV — the virus that causes nearly all cervical cancers — with around 4 in 100 also showing abnormal cell changes that need follow-up. This does not mean cervical cancer will develop. Early monitoring and treatment can prevent these cell changes from developing into cancer.
Click here to find out more from the NHS website.
Ovarian cancer
Ovarian cancer is when abnormal cells in the ovary begin to grow in an uncontrolled way. Around 7,500 women are diagnosed with ovarian cancer in the UK each year, making it the 6th most common cancer in women in the UK. The symptoms aren't always obvious, and ovarian cancer is often diagnosed late, but early diagnosis can mean it's more treatable.
-
Ovarian cancer can affect women, some transgender men, and non-binary people assigned female at birth. It mostly affects women over the age of 50, although anyone with ovaries can get ovarian cancer.
-
The symptoms of ovarian cancer are not always obvious, and women with very early stage ovarian cancer often don't have any symptoms at all. When symptoms do appear, they may be vague but can include:
Feeling bloated (having a swollen tummy)
Feeling full quickly and/or loss of appetite
Pain or discomfort in the lower tummy area and/or back
Needing to pass urine more often or more urgently
Changes in bowel habits (such as diarrhoea or constipation)
Weight gain or weight loss
Unexplained or extreme tiredness
If you have any of the symptoms listed above, particularly if:
They are not normal for you
They are persistent
There are repeated episodes (especially more than 12 times a month, or lasting more than 3 weeks)
They do not go away
…be sure to visit your GP for a check-up. If you are over 50 and develop symptoms similar to irritable bowel syndrome (IBS), such as bloating or changes in bowel habits, you should also see your GP — it's unusual to develop IBS for the first time at this age.
Remember, most women with symptoms like these do not have cancer. But your awareness of your body is the first and most important step — early diagnosis can save lives.
-
The exact cause of ovarian cancer is unknown, but several factors can increase your risk, while others may help reduce it. The NHS lists the main risk factors as:
(Risk factors are characteristics at the biological, psychological, family, community, or cultural level that precede and are associated with a higher likelihood of negative outcomes.)
01 — Getting older
The risk of developing ovarian cancer increases with age. Most cases in the UK are in women over 50, and most cases occur after the menopause.
02 — Inherited faulty genes
You may have a higher chance of getting ovarian cancer if you've inherited a faulty gene, such as the BRCA1, BRCA2, or genes linked to Lynch syndrome. These genes also increase the risk of breast and bowel cancer. If ovarian cancer runs in your family, talk to your GP — they may refer you to a specialist for genetic testing.
03 — Previous breast or bowel cancer
Having had breast cancer or bowel cancer can increase your risk of developing ovarian cancer, partly because these cancers can sometimes be linked to the same inherited gene faults.
Other factors that may increase the risk include:
Having had radiotherapy treatment for a previous cancer
Endometriosis or diabetes
Starting your periods at a young age, going through the menopause late (over 55), or not having had a baby — because these things may mean you've ovulated more
Never having used hormonal contraception (such as the pill or an implant)
Taking hormone replacement therapy (HRT)
Being overweight
Smoking
It's still possible to get ovarian cancer even if you've had your ovaries removed, because ovarian cancer can also develop in the fallopian tubes or the lining of the tummy (peritoneum).
-
Most women with a new diagnosis of ovarian cancer are treated with a combination of surgery and chemotherapy. Other treatments — including targeted medicines, radiotherapy, and hormone therapy — may also be used depending on the type and stage of cancer.
Surgery is often the main treatment when ovarian cancer is found early. Depending on where the cancer is and whether it has spread, this may involve removing one or both ovaries and the fallopian tubes (a bilateral salpingo-oophorectomy), as well as the womb and cervix (an abdominal hysterectomy). If the cancer has spread, more extensive surgery may be needed to remove as much of it as possible — sometimes including fatty tissue in the abdomen, lymph nodes, or parts of the bowel.
Chemotherapy may be given before surgery, after surgery, or on its own, and is also used if ovarian cancer comes back. Radiotherapy may be used to treat advanced cancer or to help relieve symptoms such as bleeding, pain or discomfort. Targeted therapies — medicines that only target things that help cancer cells to grow or survive — may be an option for some types of advanced ovarian cancer or cancer that has returned.
For younger women, treatment can affect fertility, and your specialist team will discuss options to preserve fertility where possible.
Your specialist care team will explain the treatments, their benefits and side effects, and work with you to create a treatment plan that's right for you. You'll have regular check-ups during and after treatment.
Click here to find out more from the NHS website.
vaginal cancer
Vaginal cancer is a very rare cancer that's found anywhere in the vagina. It's most common in women aged 75 and over. Anyone with a vagina can get vaginal cancer.
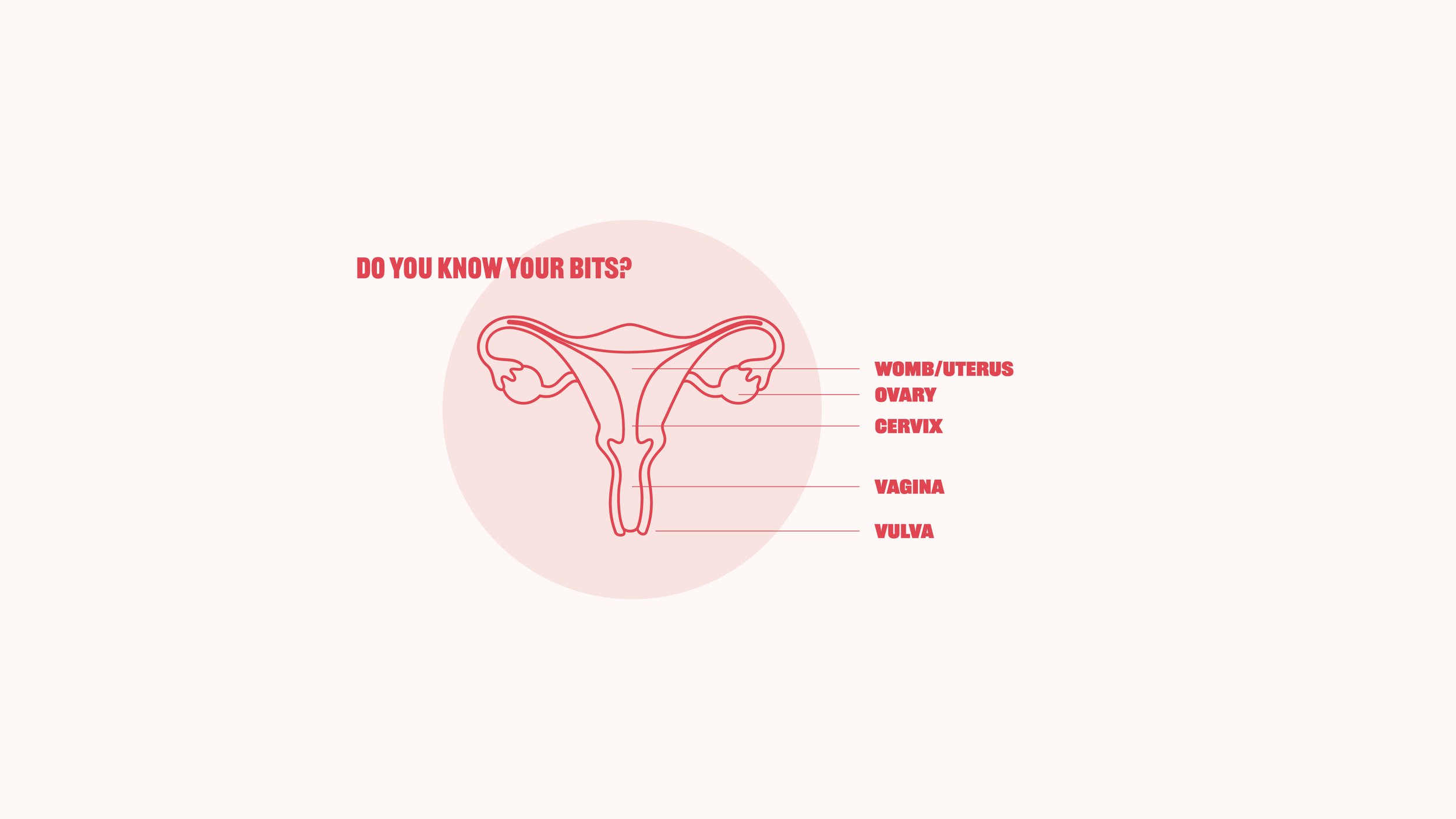
The vagina is a tube between the vulva and the opening of the womb (cervix). Check the anatomy diagram above to see where it's located!
Vaginal cancer is nearly always caused by an infection from certain types of the human papillomavirus (HPV), and usually grows very slowly. It can often be found and prevented by attending cervical screening, which aims to find and treat abnormalities before they turn into cancer. The HPV vaccine — offered to children in school and free on the NHS for anyone up to their 25th birthday — also protects against the strains of HPV most likely to cause vaginal cancer.
-
Vaginal cancer is rare, with around 250 new cases diagnosed in the UK each year. About 1 in 1,600 women in the UK will be diagnosed with vaginal cancer in their lifetime.
-
It's rare to have symptoms if you have very early vaginal cancer or abnormal cell changes in the lining of the vagina (called vaginal intraepithelial neoplasia, or VAIN). Some people have no symptoms at all, and signs of VAIN or early vaginal cancer are sometimes picked up during routine cervical screening. As with most cancers, doctors can successfully treat the disease at this early stage.
The main symptoms of vaginal cancer are:
A lump in the vagina
Ulcers or other skin changes in or around the vagina
Other symptoms include:
Bleeding between periods or after the menopause
Bleeding after sex, or pain during sex
Vaginal discharge that smells or is bloodstained
An itch in the vagina that won't go away
Pain when you pee, or needing to pee more often than usual
If vaginal cancer has spread, it can also cause:
Constipation, or feeling unable to fully empty your bowels
Swelling in your legs (oedema)
Pelvic pain that won't go away
Blood in your urine
If you have any of the symptoms above, particularly if:
They are not normal for you
They are persistent
There are repeated episodes
They do not go away
…be sure to visit your GP for a check-up.
Remember, these symptoms are very common and can be caused by many different conditions — most women with symptoms like these do not have cancer. But your awareness of your body is the first and most important step, and early diagnosis can save lives.
-
The exact cause of vaginal cancer is unknown, but several factors can increase your risk. The biggest single factor is HPV — more than half of all vaginal cancers are caused by an infection with certain types of human papillomavirus (HPV), which can be passed on through any skin-to-skin contact of the genital area, vaginal, anal or oral sex, and sharing sex toys.
(Risk factors are characteristics at the biological, psychological, family, community, or cultural level that precede and are associated with a higher likelihood of negative outcomes.)
01 — Getting older
Vaginal cancer is most common in women aged 75 and over, with risk increasing as you get older.
02 — HPV and previous abnormal cells
You're more likely to get vaginal cancer if you've had an HPV infection, or if precancerous cells have been found in your cervix (called CIN) or vagina (called VAIN). Having had cervical cancer also increases your risk.
03 — Previous womb cancer or radiotherapy
Having had womb cancer — especially if you were treated with radiotherapy — can increase your risk of developing vaginal cancer later.
Other factors that may increase the risk include:
Having lupus, HIV or AIDS, or another condition that affects your immune system
Smoking, which can weaken your immune system
Your mother having taken the hormonal medicine diethylstilbestrol (DES) while pregnant with you — your GP can discuss this with you
It's still possible to get vaginal cancer even if you've had a hysterectomy. Trans and non-binary people who have a vagina, or part of a vagina from gender surgery, can also get vaginal cancer.
How to lower your risk
You can't always prevent vaginal cancer, but because there's a strong link with HPV, the best ways to protect yourself are:
Attending cervical screening when you're invited — this finds and treats cell changes before they turn into cancer
The HPV vaccine, which is offered to all children aged 12–13 in school and is free on the NHS for anyone up to their 25th birthday
Using condoms (although these don't cover all the skin around your genitals, so don't fully protect against HPV)
Quitting smoking
Eating a balanced diet to support your immune system
-
There is no screening programme for vaginal cancer because it is very rare. However, when you have a cervical screening test, the doctor or nurse uses a speculum to see inside, and they may pick up precancerous cell changes in the vagina (called VAIN) at the same time. Treating VAIN early can prevent vaginal cancer from developing.
Vaginal cancer is often treatable. The treatment you have will depend on the size, type and location of the cancer, whether it has spread, and your general health.
The main treatment for vaginal cancer is radiotherapy, which uses high-energy rays to kill cancer cells. It can be given from outside the body (external radiotherapy) or from inside the body (a type called brachytherapy).
Surgery is usually only used if the cancer is found early, or if radiotherapy hasn't worked. Depending on the size and position of the cancer, surgery may involve removing part of the vagina, all of the vagina, or in more advanced cases, the vagina along with the cervix, womb, ovaries and fallopian tubes (a hysterectomy). If your vagina has to be removed, you can ask your surgeon about vaginal reconstruction, which uses skin and muscle from other parts of the body to create a new vagina.
Chemotherapy is rarely used on its own for vaginal cancer. It's usually given alongside radiotherapy (called chemoradiotherapy) to make the radiotherapy more effective.
Your specialist team will explain the treatments, their benefits and side effects, and work with you to create a treatment plan that's right for you. You'll have regular check-ups during and after treatment.
Click here to find out more from the NHS website.
vulvaL cancer
The vulva is the name for a woman's external genitals. It includes:
The lips surrounding the vagina (labia majora and labia minora)
The clitoris
The Bartholin's glands, two small glands on each side of the vagina
Vulval cancer can develop on any part of the vulva, but most commonly affects the inner edges of the labia. Less often, it can affect the clitoris, the Bartholin's glands, or the perineum (the skin between the vulva and the anus).
Most people affected by vulval cancer are women over the age of 65, and the condition is rare in women under 50 who have not yet gone through the menopause. Vulval cancer can affect anyone with a vulva, including trans men and non-binary people assigned female at birth.
-
Vulval cancer is rare. Around 1,400 women are diagnosed with vulval cancer in the UK each year. It is more common in older women — more than 4 in 10 cases are in women aged 75 and over, and the condition is rare in women under 50 who have not yet gone through the menopause.
Vulval cancer can affect anyone with a vulva, including trans men and non-binary people assigned female at birth.
-
Symptoms of vulval cancer can affect any part of the vulva, but they're most common on the inner and outer lips (the labia) around the opening of the vagina. Symptoms can include:
Itching that does not get better
Pain, soreness or tenderness in the vulva
Changes to your skin, such as red, white or dark patches (these may be harder to see on brown or black skin), or an area of thickened or raised skin
A lump, swelling, or wart-like growth on the vulva
A sore, ulcer or open sore on the vulva
Bleeding from your vulva, or blood-stained vaginal discharge, that is not related to your periods
A burning pain when you pee
A mole on the vulva that changes shape or colour
If you have any of the symptoms listed above, particularly if:
They are not normal for you
They are persistent
There are repeated episodes
They do not go away
…be sure to visit your GP for a check-up.
Remember, these symptoms are very common and can be caused by many different conditions — most women with symptoms like these do not have cancer. But your awareness of your body is the first and most important step, and early diagnosis can save lives.
-
The exact cause of vulval cancer isn't always known, but several factors can increase your risk.
01 — Getting older
The risk of developing vulval cancer increases with age. It mostly affects women over 65, although you can get it at any age.
02 — HPV (human papillomavirus)
HPV is thought to be responsible for around 7 in 10 vulval cancers. HPV is passed on through skin-to-skin contact of the genital area, vaginal, anal or oral sex, and sharing sex toys. Most people who have an HPV infection will not go on to develop vulval cancer — the body's immune system usually clears the virus on its own.
03 — Vulval intraepithelial neoplasia (VIN)
VIN is a precancerous condition where abnormal cell changes develop in the skin of the vulva. In some women, VIN can develop into vulval cancer if it isn't treated. The most common symptom of VIN is a lasting itch that does not get better or go away.
Other factors that may increase the risk include:
Skin conditions affecting the vulva, such as lichen sclerosus or lichen planus
A weakened immune system — for example, having HIV, or taking medicines that suppress your immune system (such as after an organ transplant)
Smoking, which can weaken the immune system and make it harder for the body to clear HPV
Having had cervical cancer — because cervical and vulval cancer share some of the same risk factors, including HPV
-
The main treatment for vulval cancer is usually surgery. You may also have radiotherapy or chemotherapy, depending on the type and size of the cancer, where it is, whether it has spread, and your general health. Sometimes a combination of treatments is used.
Surgery aims to remove the cancer along with a border of healthy tissue around it. The type and extent of surgery depends on the size and position of the cancer — this can range from removing a small affected area, to removing part of the vulva, or in some cases the whole vulva (a vulvectomy). You may also need some lymph nodes in your groin removed. After surgery, the surgeon will repair the vulva using the remaining skin, or — in some cases — a plastic surgeon will reconstruct the vulva using skin or muscle from another part of your body.
Radiotherapy uses high-energy rays to kill cancer cells. It may be given before surgery to shrink a large cancer, after surgery to lower the risk of it returning, or as an alternative if surgery isn't right for you. Chemotherapy uses medicines to kill cancer cells, and may be given alongside radiotherapy (called chemoradiotherapy). Both can also be used to relieve symptoms in advanced cases.
Your specialist team will explain the treatments, their benefits and side effects, and work with you to create a treatment plan that's right for you. You'll be supported through surgery and recovery by your specialist team.
Click here to find out more from the NHS website.
Womb (Uterus) cancer
Womb cancer is cancer that affects the womb (uterus) — the organ where a baby grows during pregnancy. It's most common in women who've been through the menopause. Womb cancer can affect anyone with a womb, including trans men and non-binary people assigned female at birth.
Most womb cancer starts in the lining of the womb (the endometrium), which is why it's also known as endometrial cancer.
Around 10,200 women are diagnosed with womb cancer in the UK each year, making it the fourth most common cancer in women in the UK (Cancer `Research UK, 2026). Cases are rising, but if caught early, womb cancer is very treatable.
-
Around 9,700 women are diagnosed with womb cancer in the UK each year, making it the fourth most common cancer in women in the UK. Around 5 out of every 100 cancers diagnosed in women are womb cancers, and cases are rising.
Womb cancer mostly affects women who have been through the menopause, with around 3 in 4 cases in women aged 60 and over. It can affect anyone with a womb, including trans men and non-binary people assigned female at birth.
By far the most common type of womb cancer is endometrial cancer, which starts in the lining of the womb (the endometrium).
-
The most common symptom of womb cancer is unusual vaginal bleeding. This includes:
Bleeding after the menopause — including any spotting, or pink, brown or red discharge
Bleeding between periods (before the menopause)
Periods that are heavier than usual for you
Vaginal discharge that's unusual for you (which can be watery, pink, or bloodstained)
Most cases of womb cancer are picked up because of unusual bleeding. If you have been through the menopause, any bleeding is not normal and should be checked, even if it's a one-off or just spotting.
Less common symptoms can include:
Pain or discomfort in the lower abdomen or pelvis
Pain during sex
Pain or discomfort when peeing
If womb cancer has spread, it can also cause:
Loss of appetite or unexplained weight loss
Tiredness or weakness
Feeling or being sick
Constipation
Feeling breathless
Needing to pee more often than usual
If you have any of the symptoms listed above, particularly if:
They are not normal for you
They are persistent
There are repeated episodes
They do not go away
…be sure to visit your GP for a check-up. Don't wait — even if you've recently had a normal cervical screening, that test only checks the cervix and rarely picks up womb cancer.
Remember, these symptoms are very common and can be caused by many different conditions — most women with symptoms like these do not have cancer. But your awareness of your body is the first and most important step, and early diagnosis can save lives.
-
The exact cause of womb cancer isn't always known, but several factors can increase your risk. Most risk factors are linked to how much oestrogen the lining of the womb is exposed to over a woman's lifetime — and around 4 in 10 womb cancers in the UK are thought to be preventable.
01 — Getting older
Womb cancer is most often diagnosed in women aged between 60 and 79, with incidence peaking in women aged 75 to 79.
02 — Oestrogen and weight
Most womb cancers are driven by the hormone oestrogen. Being overweight or obese is the biggest single modifiable risk factor for womb cancer — around 1 in 3 cases are caused by being overweight or obese. After the menopause, fat tissue is the main source of oestrogen, which is why excess weight has such a strong effect on risk.
03 — Hormonal and menstrual factors
Several hormonal and menstrual factors can increase your risk of womb cancer, including:
Starting your periods at a young age, or going through the menopause late
Never having been pregnant — having a baby lowers your risk, and having more than one lowers it further
Polycystic ovary syndrome (PCOS), which can cause higher levels of oestrogen
Taking oestrogen-only hormone replacement therapy (HRT)
Taking tamoxifen, a medicine used to treat breast cancer (the benefits of tamoxifen for breast cancer usually outweigh this risk — your doctor will discuss this with you)
04 — Other health conditions
Diabetes — having diabetes can raise oestrogen levels in the body
Lynch syndrome — an inherited condition that increases the risk of womb and bowel cancer. The NHS now tests all womb cancers for Lynch syndrome routinely.
Previous cancer — you're at slightly increased risk of womb cancer if you've previously had breast, bowel or rectal cancer. Once you've had womb cancer, you also have a slightly increased risk of certain other cancers.
-
Surgery is the main treatment for most women with womb cancer, especially when it's found early. For some women, surgery alone is enough to cure the cancer. Other treatments — including radiotherapy, chemotherapy, hormone therapy, immunotherapy or targeted medicines — may also be used depending on the type and stage of the cancer, where it is, whether it has spread, and your general health.
Surgery for womb cancer usually involves a hysterectomy — removing the womb and cervix, along with the ovaries and fallopian tubes. This is increasingly done as keyhole (laparoscopic) or robot-assisted surgery, which means a faster recovery. If the cancer has spread, more extensive surgery may be needed, sometimes including removal of nearby lymph nodes.
Radiotherapy uses high-energy rays to kill cancer cells. It may be given after surgery to lower the risk of the cancer coming back, alongside chemotherapy (chemoradiotherapy), or as the main treatment if surgery isn't right for you. A type of radiotherapy called brachytherapy — where a radioactive source is placed inside the vagina to deliver a targeted dose — is often used after surgery for womb cancer.
Chemotherapy uses medicines to kill cancer cells. It can be given alongside radiotherapy, after surgery to help stop the cancer coming back, or to slow advanced cancer. Hormone therapy may be used for advanced or recurrent womb cancer, especially if you're not well enough for surgery or radiotherapy. For some women with advanced or recurrent endometrial cancer, immunotherapy and targeted medicines (such as pembrolizumab with lenvatinib, or dostarlimab) are now also available on the NHS.
Your specialist team will explain the treatments, their benefits and side effects, and work with you to create a treatment plan that's right for you. You'll have regular check-ups during and after treatment.
Click here to find out more from the NHS website.
-
Cervical screening is one of the most effective tools we have to prevent cervical cancer. It's not a test for cancer itself — it's a test for high-risk HPV (the virus that causes nearly all cervical cancers) and, if HPV is found, for any abnormal cell changes on the cervix. Treating these cell changes early can stop cancer from developing in the first place.
-
In England, cervical screening is offered to all women and people with a cervix between the ages of 25 and 64. This includes trans men and non-binary people who have a cervix — if you're registered with your GP as female you'll be invited automatically; if you're registered as male, you can ask your GP to arrange screening for you.
-
You'll usually be invited every 5 years, or sooner (typically every 1 to 3 years) if you've previously had an abnormal result or high-risk HPV detected. You'll receive a letter when you're due — most people are first invited at age 24 and a half, so they can have their first test by age 25.
-
The screening test itself only takes a few minutes and is usually carried out at your GP practice by a trained nurse. You'll be asked to undress from the waist down, behind a screen, and lie on an examination bed. The nurse uses a smooth tube-shaped tool called a speculum to gently open the vagina, then uses a small soft brush to collect a sample of cells from the cervix. The sample is sent to a lab for testing.
It can feel uncomfortable, but it shouldn't be painful. You can ask for a female nurse, bring someone with you, ask for a smaller speculum, or stop the appointment at any time. If you have concerns about attending — for example if you've experienced trauma, have a disability, or are trans or non-binary — your GP practice can offer adjustments to make screening more accessible.
-
You'll usually receive your results by letter within four weeks. Around 13 in every 100 people screened will receive a result that detects high-risk HPV. Of these, around 4 in 100 will also show abnormal cell changes that need follow-up at a colposcopy clinic. The remaining 87 in 100 will be HPV negative and won't need any further tests until their next screening invitation. This does not mean cervical cancer will develop — early monitoring and treatment can prevent these cell changes from developing into cancer.
-
In 2023–24, over 5 million people aged 25 to 64 were invited for cervical screening in England. But around 5 million women in England are currently not up to date with their screening, which means many preventable cancers go undetected. If you've missed your invitation, you can still book an appointment with your GP at any time — it's never too late to catch up.
cervical screening
Click here to find out more from the NHS website.
-
Human papillomavirus (HPV) is a very common virus passed on through skin-to-skin contact of the genital area, including during vaginal, anal or oral sex, and through sharing sex toys. Most people will get HPV at some point in their lives, and in most cases the body clears it without any problems. But certain high-risk types of HPV can cause cancer — including nearly all cervical cancers, more than half of vaginal cancers, around 7 in 10 vulval cancers, and some anal, penile, and head and neck cancers.
-
The HPV vaccine protects against the strains of HPV most likely to cause cancer, as well as the strains that cause genital warts. It's one of the most effective cancer-prevention tools we have, and is recommended by the NHS, the World Health Organization, and the UK Health Security Agency.
-
The HPV vaccine is offered to all children in Year 8 (aged 12 to 13) in school, regardless of gender. Boys have been included in the school programme since 2019. The vaccine is also offered to:
Men aged 45 and under who have sex with men (through sexual health and HIV clinics)
People who are immunocompromised, or living with HIV
Anyone under 25 who missed the vaccine at school — available free on the NHS
-
In England, the HPV vaccine is offered in school during Year 8. Since September 2023, it's given as a single dose (it used to be two), making the programme simpler and more accessible. If you missed it at school, you can get it free on the NHS up to your 25th birthday — just contact your GP practice to book.
-
The impact has been remarkable. Cervical cancer rates among young women in England have dropped by almost 90% since the HPV vaccine was introduced — one of the strongest pieces of evidence of its kind, anywhere in the world. The vaccine is also expected to reduce rates of vaginal, vulval, anal, and some head and neck cancers as more vaccinated cohorts reach adulthood.
-
The HPV vaccine has been used in over 100 countries and has an excellent safety record. Like all vaccines, it can have mild side effects — most commonly a sore arm, headache, or feeling tired for a day or two — but serious side effects are extremely rare. Over 100 million doses have been given worldwide, and decades of monitoring have confirmed it's safe and effective.
hpv vaccine
Click here to find out more from the NHS website.
Resources
Feel free to download and use our gynaecological health resources below.
the vagina dialogues
Let’s not beat around the bush. It’s why we’ve fanny packed this little guide with lots of learning about those lovely bits between your legs. Made for university students.
5 gynae cancer factsheets
Like most cancers, the earlier you spot and treat gynae cancers, the more treatable they are - so we’ve put together some factsheets for you.
signs & symptoms poster
Knowing what's normal for you is half the battle. This poster lays out the signs and symptoms of all five gynae cancers. Perfect for the back of a loo door, a staff room, or anywhere people have a quiet minute to read.
symptom tracker
Awareness of the gynae cancer symptoms is low, and often they can be hard to recognise - it’s what makes paying attention and knowing your body’s normal so important.
HPV workplace poster
. This poster covers what HPV is, the cancers it can cause, and how to protect yourself and the people you love — designed to live on an office wall, a noticeboard, or anywhere a bit of useful info won't go amiss.